Carbohydrate Mouth Rinsing Enhances High Intensity Time Trial Performance Following Prolonged Cycling

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Cardiorespiratory Fitness
2.3. Experimental Design
2.4. Mouth Rinse Solutions
2.5. Dependent Measures
2.5.1. Cycling Performance
2.5.2. Skeletal Muscle Function
2.5.3. Heart Rate (HR), Rating of Perceived Exertion (RPE), and Blood Glucose
2.6. Dietary and Physical Activity Controls
2.7. Statistical Analysis
3. Results
3.1. Cycling Pre-Load
3.2. Mouth Rinse Effects
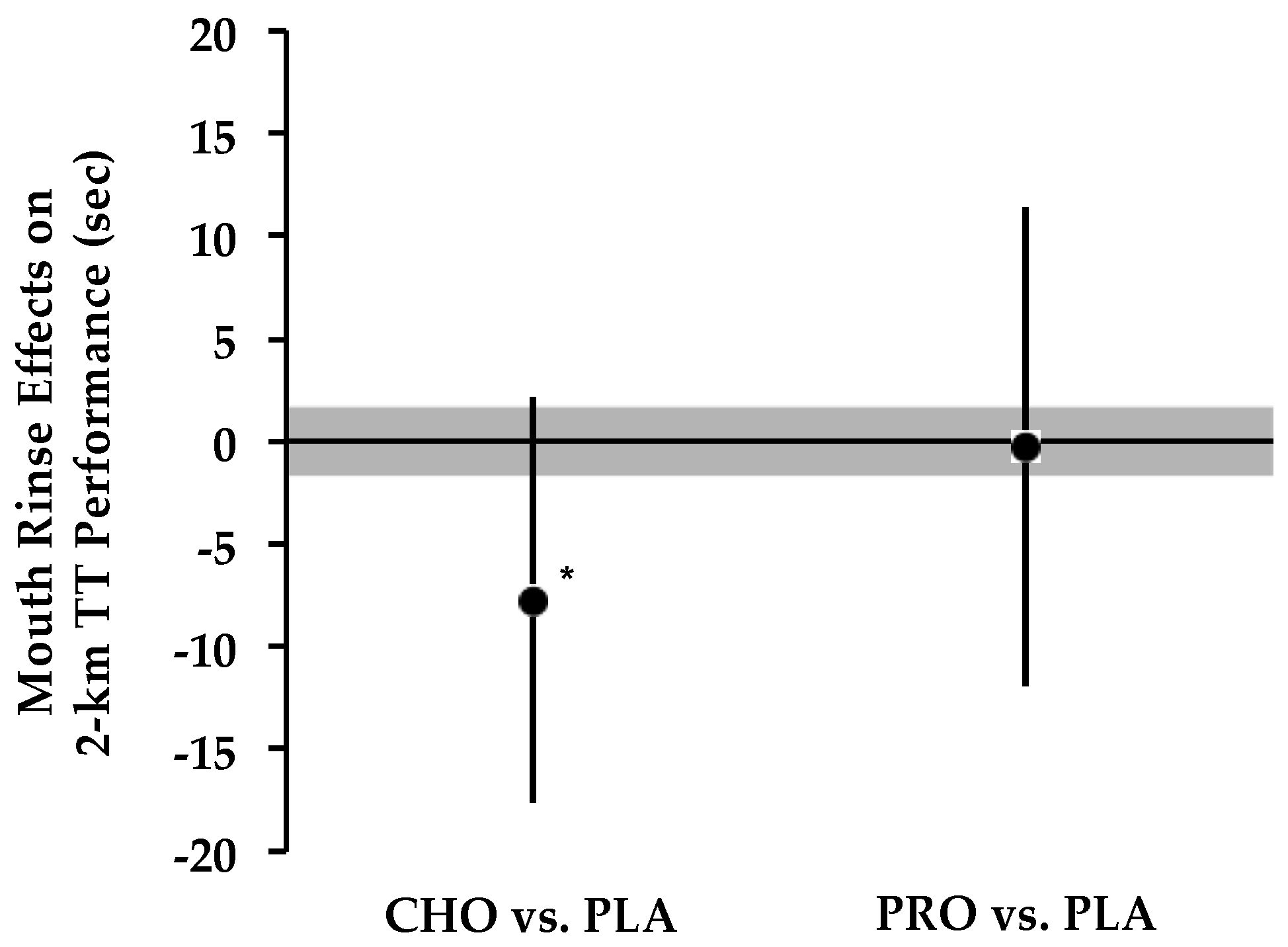
3.2.1. Performance
3.2.2. Skeletal Muscle Function
3.2.3. Heart Rate, RPE, and Blood Glucose
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Coggan, A.R.; Coyle, E.F. Reversal of fatigue during prolonged exercise by carbohydrate infusion or ingestion. J. Appl. Physiol. 1987, 63, 2388–2395. [Google Scholar] [PubMed]
- Coyle, E.F.; Hagberg, J.M.; Hurley, B.F.; Martin, W.H.; Ehsani, A.A.; Holloszy, J.O. Carbohydrate feeding during prolonged strenuous exercise can delay fatigue. J. Appl. Physiol. 1983, 55, 230–235. [Google Scholar] [PubMed]
- Jeukendrup, A.E.; Wagenmakers, A.J.M.; Stegen, J.; Gijsen, A.P.; Brouns, F.; Saris, W.H.M. Carbohydrate ingestion can completely suppress endogenous glucose production during exercise. Am. J. Physiol. Metab. 1999, 276, E672–E683. [Google Scholar]
- Neufer, P.D.; Costill, D.L.; Flynn, M.G.; Kirwan, J.P.; Mitchell, J.B.; Houmard, J. Improvements in exercise performance: Effects of carbohydrate feedings and diet. J. Appl. Physiol. 1987, 62, 983–988. [Google Scholar] [PubMed]
- Stellingwerff, T.; Boon, H.; Gijsen, A.P.; Stegen, J.H.C.H.; Kuipers, H.; Van Loon, L.J.C. Carbohydrate supplementation during prolonged cycling exercise spares muscle glycogen but does not affect intramyocellular lipid use. Pflugers Arch. Eur. J. Physiol. 2007, 454, 635–647. [Google Scholar] [CrossRef] [PubMed]
- De Bock, K.; Derave, W.; Ramaekers, M.; Richter, E.A.; Hespel, P. Fiber type-specific muscle glycogen sparing due to carbohydrate intake before and during exercise. J. Appl. Physiol. 2007, 102, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Anantaraman, R.; Carmines, A.A.; Gaesser, G.A.; Weltman, A. Effects of carbohydrate supplementation on performance during 1 hour of high-intensity exercise. Int. J. Sports Med. 1995, 16, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Below, P.R.; Mora-Rodríguez, R.; González-Alonso, J.; Coyle, E.F. Fluid and carbohydrate ingestion independently improve performance during 1 h of intense exercise. Med. Sci. Sports Exerc. 1995, 27, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Jeukendrup, A.; Brouns, F.; Wagenmakers, A.J.M.; Saris, W.H.M. Carbohydrate-electrolyte feedings improve 1 h time trial cycling performance. Int. J. Sports Med. 1997, 18, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.M.; Jeukendrup, A.E.; Jones, D.A. The effect of carbohydrate mouth rinse on 1-h cycle time trial performance. Med. Sci. Sports Exerc. 2004, 36, 2107–2111. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.S.; Bridge, M.W.; Jones, D. A Carbohydrate sensing in the human mouth: Effects on exercise performance and brain activity. J. Physiol. 2009, 587, 1779–1794. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.C.; Bird, S.R.; Burke, L.M.; Hawley, J. A Effect of a carbohydrate mouth rinse on simulated cycling time-trial performance commenced in a fed or fasted state. Appl. Physiol. Nutr. Metab. 2013, 38, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Fares, E.J.M.; Kayser, B. Carbohydrate mouth rinse effects on exercise capacity in pre- and postprandial states. J. Nutr. Metab. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Beelen, M.; Berghuis, J.; Bonaparte, B.; Ballak, S.B.; Jeukendrup, A.E.; Van Loon, L.J.C. Carbohydrate mouth rinsing in the fed state: Lack of enhancement of time-trial performance. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Ispoglou, T.; O’Kelly, D.; Angelopoulou, A.; Bargh, M.; O’Hara, J.P.; Duckworth, L.C. Mouth-rinsing with carbohydrate solutions at the postprandial state fail to improve performance during simulated cycling time trials. J. Strength Cond. Res. 2015, 29, 2316–2325. [Google Scholar] [CrossRef] [PubMed]
- Trommelen, J.; Beelen, M.; Mullers, M.; Gibala, M.J.; Van Loon, L.J.C.; Cermak, N.M. A sucrose mouth rinse does not improve 1-Hr cycle time trial performance when performed in the fasted or fed state. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Ataide-Silva, T.; Ghiarone, T.; Bertuzzi, R.; Stathis, C.G.; Leandro, C.G.; Lima-Silva, A.E. CHO mouth rinse ameliorates neuromuscular response with lower endogenous CHO stores. Med. Sci. Sport Exerc. 2016, 48, 1810–1820. [Google Scholar] [CrossRef] [PubMed]
- Rollo, I.; Williams, C.; Gant, N.; Nute, M. The influence of carbohydrate mouth rinse on self-selected speeds during a 30-min treadmill run. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 585–600. [Google Scholar] [CrossRef] [PubMed]
- Rollo, I.; Cole, M.; Miller, R.; Williams, C. The influence of mouth-rinsing a carbohydrate solution on 1 h running performance. Med. Sci. Sports Exerc. 2009, 42, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Bastos-Silva, V.J.; de Albuquerque Melo, A.; Lima-Silva, A.E.; Moura, F.A.; Bertuzzi, R.; de Araujo, G.G. Carbohydrate mouth rinse maintains muscle electromyographic activity and increases time to exhaustion during moderate but not high-intensity cycling exercise. Nutrients 2016, 8, 49. [Google Scholar] [CrossRef] [PubMed]
- Kulaksız, T.N.; Koşar, Ş.N.; Bulut, S.; Güzel, Y.; Willems, M.E.T.; Hazir, T.; Turnagöl, H.H. Mouth rinsing with maltodextrin solutions fails to improve time trial endurance cycling performance in recreational athletes. Nutrients 2016, 8, 269. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Yoo, M.J.Y.; Moss, C.; Breier, B.H. Carbohydrate mouth rinsing has no effect on power output during cycling in a glycogen-reduced state. J. Int. Soc. Sports Nutr. 2016, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.; Guelfi, K.J.; Fournier, P.A. Effect of a carbohydrate mouth rinse on maximal sprint performance in competitive male cyclists. J. Sci. Med. Sport 2011, 14, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Přibyslavská, V.; Scudamore, E.M.; Johnson, S.L.; Green, J.M.; Stevenson Wilcoxson, M.C.; Lowe, J.B.; O’Neal, E.K. Influence of carbohydrate mouth rinsing on running and jumping performance during early morning soccer scrimmaging. Eur. J. Sport Sci. 2016, 16, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Kasper, A.M.; Cocking, S.; Cockayne, M.; Barnard, M.; Tench, J.; Parker, L.; McAndrew, J.; Langan-Evans, C.; Close, G.L.; Morton, J.P. Carbohydrate mouth rinse and caffeine improves high-intensity interval running capacity when carbohydrate restricted. Eur. J. Sport Sci. 2016, 16, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Ivy, J.; Res, P.; Sprague, R.; Widzer, M. Effect of a carbohydrate-protein supplement on endurance performance during exercise of varying intensity. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 382–395. [Google Scholar] [CrossRef] [PubMed]
- Ferguson-Stegall, L.; McCleave, E.L.; Ding, Z.; Kammer, L.M.; Wang, B.; Doerner, P.G.; Liu, Y.; Ivy, J.L. The effect of a low carbohydrate beverage with added protein on cycling endurance performance in trained athletes. J. Strength Cond. Res. 2010, 24, 2577–2586. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.J.; Moore, R.W.; Kies, A.K.; Luden, N.D.; Pratt, C.A. Carbohydrate and protein hydrolysate coingestions improvement of late-exercise time-trial performance. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 136–149. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.; Luden, N.; Herrick, J. Consumption of an oral carbohydrate-protein gel improves cycling endurance and prevents postexercise muscle damage. J. Strength Cond. Res. 2007, 21, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.J.; Kane, M.D.; Todd, M.K.; Kent Todd, M. Effects of a carbohydrate-protein beverage on cycling endurance and muscle damage. Med. Sci. Sports Exerc. 2004, 36, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Gam, S.; Guelfi, K.J.; Fournier, P.A. Opposition of carbohydrate in a mouth-rinse solution to the detrimental effect of mouth rinsing during cycling time trials. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.A.; Schroer, A.B.; Luden, N.D.; Womack, C.J.; Smyth, S.A.; Saunders, M.J. Glucose-fructose enhances performance versus isocaloric, but not moderate, glucose. Med. Sci. Sports Exerc. 2014, 46, 1778–1786. [Google Scholar] [CrossRef] [PubMed]
- Gilson, S.F.; Saunders, M.J.; Moran, C.W.; Moore, R.W.; Womack, C.J.; Todd, M.K. Effects of chocolate milk consumption on markers of muscle recovery following soccer training: A randomized cross-over study. J. Int. Soc. Sports Nutr. 2010, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. How to Interpret Changes in an Athletic Performance Test. Available online: http://www.sportsci.org/jour/04/wghtests.htm (accessed on 5 September 2015).
- Paton, C.C.D.; Hopkins, W.G.W. Variation in performance of elite cyclists from race to race. Eur. J. Sport Sci. 2006, 6, 25–31. [Google Scholar] [CrossRef]
- Hopkins, W.G.W.G. A spreadsheet for deriving a confidence interval, mechanistic inference, and clinical inference from a p value. Sport Sci. 2007, 11, 16–19. [Google Scholar]
- Pottier, A.; Bouckaert, J.; Gilis, W.; Roels, T.; Derave, W. Mouth rinse but not ingestion of a carbohydrate solution improves 1-h cycle time trial performance. Scand. J. Med. Sci. Sport. 2010, 20, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Painelli, V.S.; Roschel, H.; Gualano, B.; Del-Favero, S.; Benatti, F.B.; Ugrinowitsch, C.; Tricoli, V.; Lancha, A.H. The Effect of carbohydrate mouth rinse on maximal strength and strength endurance. Eur. J. Appl. Physiol. 2011, 111, 2381–2386. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.; Stellingwerff, T.; Klimstra, M. Carbohydrate mouth rinse counters fatigue related strength reduction. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Jeffers, R.; Shave, R.; Ross, E.; Stevenson, E.J.; Goodall, S. The effect of a carbohydrate mouth-rinse on neuromuscular fatigue following cycling exercise. Appl. Physiol. Nutr. Metab. 2015, 40, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Gant, N.; Stinear, C.M.; Byblow, W.D. Carbohydrate in the mouth immediately facilitates motor output. Brain Res. 2010, 1350, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, J.; Bottoms, L.; Flynn, C.; Bradley, E.; Alexander, G.; McCullagh, S.; Finn, T.; Hurst, H.T. The effect of different durations of carbohydrate mouth rinse on cycling performance. Eur. J. Sport Sci. 2014, 14, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.; Nichols, D.; Cordery, P. Mouth rinsing with a carbohydrate solution does not influence cycle time trial performance in the heat. Appl. Physiol. Nutr. Metab. 2014, 39, 1064–1069. [Google Scholar] [CrossRef] [PubMed]
- Hofman, D.L.; Van Buul, V.J.; Brouns, F.J.P.H. Nutrition, health, and regulatory aspects of digestible maltodextrins. Crit. Rev. Food Sci. Nutr. 2016, 56, 2091–2100. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, S.M.; Gelb, A.; Girvin, J.P.; Hachinski, V.C. Cardiovascular effects of human insular cortex stimulation. Neurology 1992, 42, 1727–1732. [Google Scholar] [CrossRef] [PubMed]
- Felig, P.; Cherif, A.; Minagawa, A.; Wahren, J. Hypoglycemia during prolonged exercise in normal men. N. Engl. J. Med. 1982, 306, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Flynn, M.G.; Costill, D.L.; Hawley, J.A.; Fink, W.J.; Neufer, P.D.; Fielding, R.A.; Sleeper, M.D. Influence of selected carbohydrate drinks on cycling performance and glycogen use. Med. Sci. Sports Exerc. 1987, 19, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Stebbins, C.L.; Moore, J.L.; Casazza, G.A. Effects of cadence on aerobic capacity following a prolonged, varied intensity cycling trial. J. Sport. Sci. Med. 2014, 13, 114–119. [Google Scholar]



{kind=link}
{kind=link}
| Condition | Heart Rate (bpm) | RPE | Blood Glucose (mg/dL) | Finishing Time (min) |
|---|---|---|---|---|
| Placebo | 150 ± 14 | 16 ± 1 | 68 ± 80 | 57.02 ± 5.21 |
| Carbohydrate | 148 ± 14 | 16 ± 1 | 68 ± 70 | 57.04 ± 2.75 |
| Protein | 144 ± 15 | 16 ± 1 | 66 ± 10 | 57.89 ± 7.38 |
| Condition | ∆ MVC (N) | Constant-Load—55% Wmax | 2 km TT Finishing Time (s) | ||
|---|---|---|---|---|---|
| Heart Rate (bpm) | RPE | Blood Glucose (mg/dL) | |||
| PLA | 34 ± 40 | 150 ± 13 | 14 ± 20 | 59 ± 8 | 200.1 ± 10.8 |
| CHO | 25 ± 25 | 156 ± 10 * | 14 ± 20 | 63 ± 7 ** | 192.4 ± 8.2 †† |
| PRO | 10 ± 26 ‡ | 152 ± 60 | 14 ± 3 | 56 ± 10 † | 199.9 ± 18.4 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luden, N.D.; Saunders, M.J.; D’Lugos, A.C.; Pataky, M.W.; Baur, D.A.; Vining, C.B.; Schroer, A.B. Carbohydrate Mouth Rinsing Enhances High Intensity Time Trial Performance Following Prolonged Cycling. Nutrients 2016, 8, 576. https://doi.org/10.3390/nu8090576
Luden ND, Saunders MJ, D’Lugos AC, Pataky MW, Baur DA, Vining CB, Schroer AB. Carbohydrate Mouth Rinsing Enhances High Intensity Time Trial Performance Following Prolonged Cycling. Nutrients. 2016; 8(9):576. https://doi.org/10.3390/nu8090576
Chicago/Turabian StyleLuden, Nicholas D., Michael J. Saunders, Andrew C. D’Lugos, Mark W. Pataky, Daniel A. Baur, Caitlin B. Vining, and Adam B. Schroer. 2016. "Carbohydrate Mouth Rinsing Enhances High Intensity Time Trial Performance Following Prolonged Cycling" Nutrients 8, no. 9: 576. https://doi.org/10.3390/nu8090576